Mount Sinai IV tNK Tool Protocol
IV TNK CHECKLIST
All boxes in this section must be checked to give IV TNK.
If you are unable to check any box, IV TNK is not appropriate.
Diagnosis of acute ischemic stroke
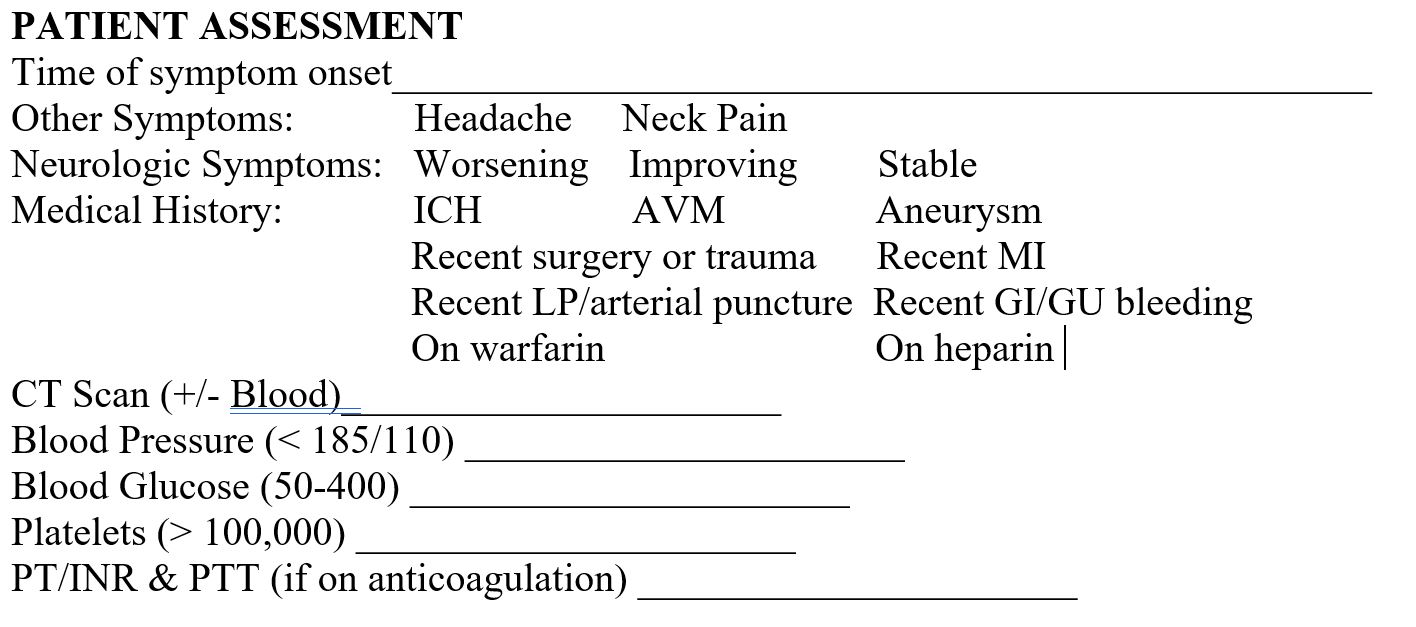
Definite time of onset
Diagnosis of ischemic stroke causing measurable neurologic deficit
Non-contrast CT head showing no hemorrhage or well-established new infarct
Onset of acute stroke symptoms is within 3 hours. Between 3 and 4.5 hours from symptom onset, selected patients may be eligible for treatment with IV alteplase, at the discretion of the treating vascular neurologist.
IV TNK is contraindicated when (one or more are selected):
Systolic BP < 185 and Diastolic BP < 110
No history of intracranial hemorrhage, brain aneurysm, AVM, or brain tumor
No intracranial or spinal surgery, head trauma, myocardial infarction or stroke within the last 3 months
No gastrointestinal or genitourinary hemorrhage within the last 21 days
No major surgery or trauma within the last 14 days
No arterial puncture at a non-compressible site within the last 7 days
No lumbar puncture within the last 3 days
No active bleeding or fracture on examination
Platelets > 100,000/mm3, PTT within normal range after dabigatran or IV heparin use, INR ≤ 1.7, and no other known bleeding diathesis
No suspicion of subarachnoid hemorrhage by imaging or clinical presentation
Patient and/or family understand the potential risks and benefits of treatment
ADDITIONAL IV TNK CHECKLIST
FOR PATIENTS TREATED BETWEEN 3 AND 4.5 HOURS All boxes in this section must be checked in addition to those above to give IV tPA in the 3 to 4.5 hour window. (based on exclusion/inclusion criteria in ECASS III)
Age < 80
No history of prior stroke and diabetes
No anticoagulant use prior to admission (even if INR ≤ 1.7)
NIHSS < 25
IV tPA CHECKLIST
RELATIVE CRITERIA FOR ADMINISTRATION IN THE 0 TO 4.5 HOUR WINDOW If all boxes below cannot be checked, a relative contraindication to IV tPA exists.
No witnessed seizure at onset
Blood glucose between 50 and 400
No increased risk of bleeding due to comorbid conditions
No rapidly resolving neurological deficits
Stroke severity not too mild (e.g., no minor or isolated neurological deficits)
MOUNT SINAI STROKE CENTER IV tPA PATIENT MANAGEMENT TOOL
PAGE 2 UPDATED MAY 2011
BLOOD PRESSURE MANAGEMENT RECOMMENDATIONS PRE-IV TNK
For SBP > 185 or DBP > 110 on 2 readings 10-15 minutes apart:
Labetalol 10 to 20 mg IV over 1-2 minutes. Can repeat dose one time; OR
Nicardipine infusion—Initiate therapy at 5 mg/hr (50 mL/hr), increase by 2.5 mg/hr every 5-15 minutes to a maximum dose of 15 mg/hr; decrease dose to 3 mg/hr when goal BP reached; OR
Last resort: Nitropaste 1 to 2 inches transdermal (Warning: Can cause precipitous blood pressure drops and headache).
Monitor BP at least every 15 minutes during antihypertensive therapy.
PRE-IV tPA PATIENT MANAGEMENT
Prior to IV tPA administration:
Make sure that the patient has 2 IVs.
Ensure that all invasive procedures, including placement of central venous access and arterial punctures, are completed and that all indwelling lines and tubes, including NG tubes and foley catheters, are inserted. Do not delay IV tPA administration to place an NG tube, foley catheter, or additional IV line.
IV tPA ADMINISTRATION
Give 0.9 mg/kg (maximum of 90 mg) tPA (alteplase, Activase) infused over 60 minutes with 10% of the total dose administered as an initial intravenous bolus over 1 minute (1 lb = 0.45 kg).
Beginning with administration of the tPA bolus, vital signs and neurologic assessments must be performed and documented by the nurse on the tPA Flowsheet:
Every 15 minutes x 2 hours (includes the hour of IV tPA administration)
Then every 30 minutes x 6 hours
Then every 60 minutes x 18 hours
Be sure to designate and communicate to the nurse a cardinal sign (one aspect of the NIH stroke scale other than level of consciousness or motor function) to be monitored on the tPA Flowsheet for worsening or improvement.
BLOOD PRESSURE MANAGEMENT RECOMMENDATIONS DURING AND POST IV tPA ADMINISTRATION
For SBP > 180 or DBP > 105 on 2 readings 10-15 minutes apart:
Labetalol 10 to 20 mg IV over 1-2 minutes. The dose may be repeated or doubled every 10 minutes to a maximum dose of 300 mg; OR
Nicardipine infusion for persistently elevated BP—Initiate therapy at 5 mg/hr (50 mL/hr), increase by 2.5 mg/hr every 5 minutes to a maximum dose of 15 mg/hr, decrease dose to 3 mg/hr when goal BP reached.
Monitor BP at least every 15 minutes during antihypertensive therapy.
POST-IV TNK PATIENT MANAGEMENT
Use the Epic post-TNK admission order set to admit patients who received IV tPA
Monitor for signs and symptoms of CNS hemorrhage, including:
Neurologic deterioration
Development of severe headache
Sudden elevation of blood pressure
New onset of nausea and vomiting Maintain SBP < 180 and DBP < 105 For 24 hours after IV TNK administration, avoid:
Placement of central venous access
Arterial punctures
Insertion of NG tubes or foley catheters
Ordering anticoagulants, antiplatelets, or NSAIDs For VTE prophylaxis in the 24 hour period after IV TNK administration:
Order sequential compression devices (flowtrons), unless a contraindication is documented